I hope this isn't the beginning of the end of wastewater testing for #COVID19 and other infectious illness.
San Diego Union-Tribune · DOGE cuts shut down San Diego County’s wastewater testing system

I hope this isn't the beginning of the end of wastewater testing for #COVID19 and other infectious illness.
After reaching a preliminary agreement last week, countries hope more than three years of negotiations on battling future pandemics will finally end. https://www.japantimes.co.jp/news/2025/04/15/world/politics/pandemic-treaty-talks-accord/?utm_medium=Social&utm_source=mastodon #worldnews #politics #covid19 #who

Heute vor vier Jahren, am 15. April 2021, war ich sehr froh: Ich konnte den Termin für meine erste Sars-CoV-2-Impfung buchen!
Die erste Tranche von Terminen, für die ich in Frage gekommen bin, wurde damals freigeschaltet. Die Termine waren ab Montag, ich hab quasi sofort reagiert, und trotzdem war mein Termin am Dienstag Nachmittag, so groß war damals die Nachfrage.
Meine Eltern (Gruppe 65+) hatten zu dem Zeitpunkt bereits die erste Teilimpfung, und meine Großmutter (90+) beide. Davor war die Phase mit den Bürgermeistys, erinnert ihr euch? Szenen haben sich abgespielt, weltweit! Es wurde gelogen und betrogen, um schneller an die Impfung zu kommen.
"Sie haben soeben beim Impfservice Wien Ihre Termine für die zwei Teilimpfungen der Corona-Schutzimpfung vereinbart. Dieses Mail enthält alle Termininformationen zur *ersten Teilimpfung* der Corona-Schutzimpfung. Die
Termindetails zur zweiten Teilimpfung erhalten Sie zeitgerecht in einem weiteren Mail vom Impfservice Wien..."
Die ersten Impfungen waren alle im Austria Center, im Untergeschoß unter dem Vorplatz, mit der Voranmeldung oben an Containern unter dem Flugdach. Memories!
From Germany:
Abnormal Coronary Vascular Response in Patients with #LongCOVID Syndrome – a Case-Control Study Using Oxygenation-Sensitive Cardiovascular Magnetic Resonance
https://www.sciencedirect.com/science/article/pii/S1097664725000523
Image is from latest Science for ME weekly update
Hashtags:
@longcovid
#PASC #PwLC #postcovid #postcovid19 #LC #Covidlonghaulers #PostCovidSyndrome #longhaulers #COVIDBrain #NeuroPASC
@covid19 #Coronavirus
#COVID19 #COVID #COVID_19 #COVIDー19 #SARSCoV2 #CovidIsNotOver
@auscovid19 #auscovid19
1/

Is COVID-19 rewriting the rules of aging? Brain decline alarms doctors.
@WSJ reports: "Millions of long-COVID patients continue to struggle with cognitive difficulties."
Gift link: https://flip.it/Rvi2S0
You know when the Wall Street Journal starts publishing news stories on #COVID19 brain damage, it might be time to pay attention. Don't use your brain? No problem, then!
"Studies have found that older people who have Covid-19 are at increased risk of developing Alzheimer’s sooner than if they haven’t had it... It doesn’t look in older adults that this is a reversible process.”
Link to WSJ article: https://www.wsj.com/health/wellness/is-covid-rewriting-the-rules-of-aging-brain-decline-alarms-doctors-6ed3dfaa
Link for those without WSJ access: http://archive.today/WxF2Z
@pathfinder @cesarpose @actuallyautistic And what they never seem to get is that such behavior can remove the WISH to associate with them. They can't imagine that anyone who can enjoy socializing would ever lose the desire for it. They assume that the motivation for seclusion must be fear. No, it's anger and disgust. I no longer CARE whether I would be able to defend myself from #COVID19 in public. I simply don't want to socialize with them anymore, whether I would be able to do so safely or not.
#FYI #US #USA #disease #diseases #AMA #AmericanMedicalAssociation #AndreaGarcia #ToddUnger #measles #covid19 #sarscov2 #covid #longcovid #mentalhealth #influenza #flu
Is flu season over? What helps allergies at home? Are there long-term effects of COVID? Do people get sick more often after COVID? Why kids should have phones?
@pathfinder @cesarpose @actuallyautistic Except for work, and my immediate household, I've been avoiding people since the start of #COVID19. The lack of full solidarity against the disease has been intensely alienating. Why should I want to associate with those who would happily infect me with a disease that could leave me maimed or dead?
By comparison, here is a photo taken by my wife in December 2019 — one of the last few times we dined out. I don't think I look much like a misanthrope by nature. But the public reaction to #COVID19 has made me one.

With the LP.8.1.* variant on the way to dominance in most places, it is time to ponder which variant might drive the next wave.
The leading contenders at this point are LF.7.7.2, LF.7.9, NB.1.8.1, NY.9 (new), XEC.25.1, XFG and XFJ.
I show them here using a log scale, so you can compare their growth rates vs the most common LP.8.1.* sub-lineage: LP.8.1.1. Note the recent sample volumes are quite low, so the right side of this chart might not be a representative picture.

https://www.europesays.com/uk/17090/ Cheapest European cities to fly to in 2025 #Coronavirus #COVID19 #EU #Europe #European

RT @EckerleIsabella@x.com: »My opinion & I will die on this hill: The current anti-vaccine movement will have a major impact on women and will reverse women's rights. When women have to produce extra babies because 1 in 5 will not survive, they will not have energy or time to fight for equality anymore.
While being pregnant, postpartum, caring for many children, caring for a sick child, grieving deceased ones & fearing their siblings dying as well, women will be drained of energy & will not fight oppression. Without vaccines, a lot of healthy children will not survive their early childhood period.
In addition, not providing vaccines will disproportionally affect vulnerable children: While many perfectly healthy children will die, those with underlying conditions are even at higher risk. Not protecting them will shorten their life. We've seen it already during Covid.
I just want to stress this: Most of society is not aware in which a luxury situation vaccines has put parents in only the last few decades, that is, not seeing your young children die. If you don't believe me, read books about the polio period, or visit an old graveyard. It's all there.«
STUDY finds that the Novavax #COVID19 vaccine may provide more robust protection against medically attended COVID-19, compared to Pfizer.
https://www.medrxiv.org/content/10.1101/2025.04.11.25325672v1
So, of course, our HHS secretary is casting doubt on the Novavax vaccine effectiveness and its likelihood of approval this year.

World Health Organization members on Saturday reached an agreement over how to tackle future pandemics after three years of discussions. https://www.japantimes.co.jp/news/2025/04/13/world/science-health/future-pandemic-accord/?utm_medium=Social&utm_source=mastodon #worldnews #sciencehealth #who #diseases #health #covid19

The CDC wrote its own elitaph by sneering, condescending at & ultimately dismissing #covid19 & airborne viral transmission advocates, letting Delta Airlines set public health policy, & ultimately being an agency captured & purposed to be subservient primarily to the ruling class.
Walensky et al can roast in hell.
This isnt a good thing of course -- millions will suffer.
But it was in large part because of their actions that it is so.
And yeah, I recall all those houses at Halloween in Atlanta mocking citizens for "doing their own research".
After tacitly suggesting we do just that -- "do your own risk assessment".
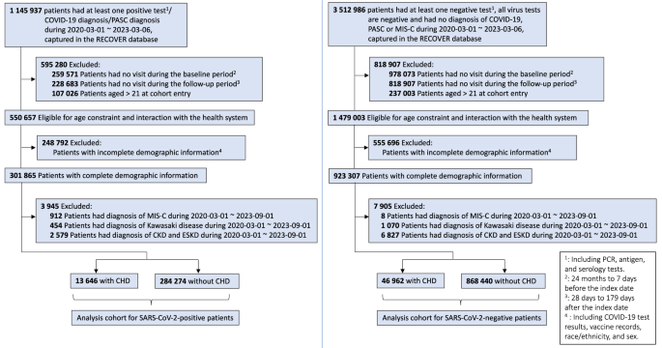
#CovidIsNotOver and it increases the risk of cardiovascular post-acute sequelae in kids
https://www.nature.com/articles/s41467-025-56284-0
Another passage that speaks volumes for me since #covid19. Way before really, Iraq War probably; but never so explicitly conclusive.
"None of us got here overnight. There are stages to the process of being betrayed by your society. One is jolted from complacency by the discovery of difference, by hypocrisy, by inexplicable or incongruous ill treatment.
What follows is a time of confusion -- deconstructing & unlearning what one thought to be the truth. Immersing oneself in the new truth. And then a decision must be made.
Some accept their fate. Swallow their pride, forget the real truth, embrace the falsehood for all they're worth -- because, they decide, they cannot be worth much. If a whole society has dedicated itself to their subjugation after all, then surely they deserve it. Even if they dont, fighting back is too hard, too painful, too impossible. At least this way, there is peace of a sort. Fleetingly.
The alternative is to demand the impossible. To change society [& the prevailing unjust world order]. There can be peace this way too.
But not before conflict."
- NK Jemisin
that Blood Advances paper aligns with earlier autopsy results, and confirmed
SARS-CoV-2+ megakaryocytes are present in lung and brain autopsy tissues from deceased donors who had COVID-19
But heck! We already knew MKs were long-term impacted. This from 2024 https://ashpublications.org/bloodadvances/article/8/11/2777/515445/SARS-CoV-2-infection-modifies-the-transcriptome-of - though in mice gives what I guess should be an obvious outcome, since the immune system isn't open-loop:
Megakaryocytes (MKs), integral to platelet production, predominantly reside in the bone marrow. [...] at peak SARS-CoV-2 viremia, when the disease primarily affected the lungs, MKs were not significantly different from those from healthy mice. Conversely, a significant divergence in the MK transcriptome was observed during systemic inflammation, although SARS-CoV-2 RNA was never detected in the BM, and it was no longer detectable in the lungs. Under these conditions, the MK transcriptional landscape was enriched in pathways associated with histone modifications, MK differentiation, NETosis, and autoimmunity
and autoimmunity
The breadcrumbs are everywhere.
fin/

That aligns with results from 2022-2023 like https://ashpublications.org/bloodadvances/article/7/15/4200/494910/Circulating-SARS-CoV-2-megakaryocytes-are which found
Using peripheral blood, we show that megakaryocytes are increased in the systemic circulation in COVID-19
peripheral blood - circulating!!
SARS-CoV-2–containing megakaryocytes are a strong risk factor for mortality and multiorgan injury
2/

So. How about this careful result demonstrating viral replication inside megakaryocyte immune cells?
transmission electron microscopy pointed to the presence of viral particles inside bone marrow MK. Immunolabeling confirmed the presence of two SARS-CoV-2 proteins, spike and Orf3a, as well as double-stranded RNA suggesting a potential viral replication cycle.
Note this study is from last month, but it's from hospitalized 2020-2021 patient data. It's existence proof, not population statistics.
That said:
bone marrow MK infection is not a strict determinant of mortality. However, all survivors experienced post-acute sequelae SARS-CoV-2 condition (PASC) diagnosed during post-intensive care follow-up
short